With advances in digital scope technology, urologists have been increasingly successful in navigating and irrigating the kidney to locate and treat kidney stones. Yet rates of sepsis following ureteroscopic procedures were recently reported to be a concerning 5.6 percent.
With these adverse events largely associated with pyelovenous backflow from increased intrarenal pressures during irrigation, FDA approval of the LithoVue Elite single-use ureteroscope may lessen the risk considerably by monitoring pressure levels in real time inside the kidney.
“Those of us who specialize in kidney stone treatment have always thought that intrarenal pressures were important in the risk for infectious complications and perhaps even postoperative pain, but the ability to consistently and reliably measure pressure has eluded us until the advent of this scope,” said urologist Nicole Miller, M.D., an expert in the treatment of kidney stones at Vanderbilt University Medical Center.
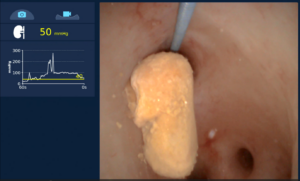
Miller demonstrated the use of this new ureteroscope in a semi-live surgery video presented at the American Urological Association Annual Meeting in May 2024. She highlighted its ability to provide enhanced digital visualization and 270-degree scope deflection in both directions and its “smart” console that allows customization of maximal intrarenal pressure and modulated irrigation inflow along with a display of real-time intrarenal pressure.
“The ability to consistently and reliably measure pressure has eluded us until the advent of this scope.”
Insights for Surgeons
When pyelovenous backflow occurs, bacteria that may be in the urine backs up into the bloodstream, allowing the release of endotoxins and renal and systemic end-organ damage from sepsis.
“We know the risk of sepsis following ureteroscopy, but we haven’t known what factors of the ureteroscopic procedure are most likely to raise intrarenal pressure,” Miller said. “We have used primitive devices to measure intrarenal pressure in animal studies and have extrapolated the data from these studies to humans, essentially making educated guesses on the pressures we are exerting on human kidneys during lithotripsy.”
The new ureteroscope also enables surgeons to test different types of irrigation systems used.
“Now, we can measure the pressures they generate,” Miller explained. “For instance, we have found that the commonly used manual syringe irrigation and single-action pump irrigation both generate very high intrarenal pressures.”
Personalizing Pressures
This pressure-measurement capability will provide data needed to enhance research into the effects of variable pressure applications during the procedure. It also will enable refinement of ureteral-access sheath sizes to personalize the procedure for each patient.
For example, Miller says the new scope may show that a 10/12 French ureteral-access sheath will not lower intrarenal pressure as well as a ureteral-access sheath of 11/13 French or above.
“We have always considered the ratio between the size of the ureteroscope and the size of the ureteral-access sheath, as this impacts irrigation outflow from the kidney,” she said. “But with real-time intrarenal pressure monitoring, we can make more informed equipment choices.”
Optimizing these procedures may lead to appropriate adjustments for various races or ethnicities. In fact, the first human trial of the LithoVue Elite showed that people of Asian ethnicity have a higher risk for excessive intrarenal pressure.
“I think this may be due to differences in the size and configuration of the intrarenal collecting system, and how perinephric fat content and lean muscle mass affect intrarenal pressure. We are beginning to realize that it’s not as simple as just the mechanics of the procedure,” Miller said.
Focus on Patients
FDA approval of the device is based on bench and preclinical results, but Miller says Vanderbilt hopes to engage soon in a multicenter trial to investigate infection-rate reduction and delineate parameters for sheath size and pressure ranges for various patient populations.
“This offers us, for the first time, a human-based research platform, so we can develop data to offer personalized medicine,” she said.
A pass-through code was developed for the LithoVue Elite that allows hospitals to be reimbursed for its use with Medicare patients.
The Southeast region of the U.S. has the highest incidence of kidney stones, thus five endourologists at Vanderbilt are kidney stone experts, devoting their time to ureteroscopy with laser lithotripsy.
“At Vanderbilt, we disproportionately see patients with more complex stones, precisely those who would benefit most from this type of intrarenal pressure monitoring,” Miller said. “So, it is particularly important that we lead efforts to improve surgical outcomes.”
“I expect the capability of measuring intrarenal pressures will improve surgeon confidence in safely performing these procedures in even the highest risk patients.”



