Treating scoliosis, particularly in young children, is fraught with difficult decision points where treatment strategy, timing and parental buy-in all factor into the success of straightening their spines.
Craig Louer, M.D., an assistant professor of orthopaedics at Monroe Carell Jr. Children’s Hospital at Vanderbilt, spearheads research into rare and severe infantile and early onset forms of scoliosis. His ongoing work is helping to clarify the decision points for these patients and drive the development of hospital and surgical protocols at Children’s Hospital.
“Nowhere is early intervention more pivotal than with these infants and young children,” Louer said. “Unlike adolescent scoliosis, early onset scoliosis can be a fatal disease if the deformity is severe enough to compromise lung function or cause right heart failure. If we identify the deformity early, we can work to maintain the curve and halt a dangerous progression.”
Poised to Intervene
Adolescent idiopathic scoliosis comprises the vast majority of pediatric scoliosis cases. For these patients, the clinical approach to mild to moderate curvatures is to observe or brace. In severe cases, the gold standard is spinal fusion at the curves.
For younger patients, however, the disease path is somewhat different. “The majority of infantile scoliosis is mild or a function of positioning or posture and may resolve on its own,” Louer said.
Knowing when to wait and watch versus when to intervene is crucial. In some children, there is an urgent race against the clock. “If it progresses, scoliosis can tremendously restrict the thoracic cavity, resulting in restricted air movement through the lungs,” Louer said. “We need to treat progressive curves of around 30 degrees as soon as we recognize them as being problematic – as early as one year of age.”
Casting as Cure or Stabilizer
Casting is still the most common treatment choice for this younger group. “In patients who are two years old or younger, a series of repeated casts over the course of 12 to 18 months is curative in roughly half of cases,” Louer explained.
“Unlike adolescent scoliosis, early onset scoliosis can be a fatal disease if the deformity is severe enough to compromise lung function or cause right heart failure.”
“It seems like the oldest technology in the world, but it has only recently become a mainstay in the treatment of early onset scoliosis. My peers generally agree it is more effective than bracing, but we need to test this.”
To that end, Vanderbilt is participating in a clinical trial comparing casting versus bracing for 440 children less than three years of age with idiopathic early onset scoliosis. “We will see what effect each is having on the curve, and also learn more about parental and patient quality of life issues in caring for these children,” Louer said.
Traction Benefits
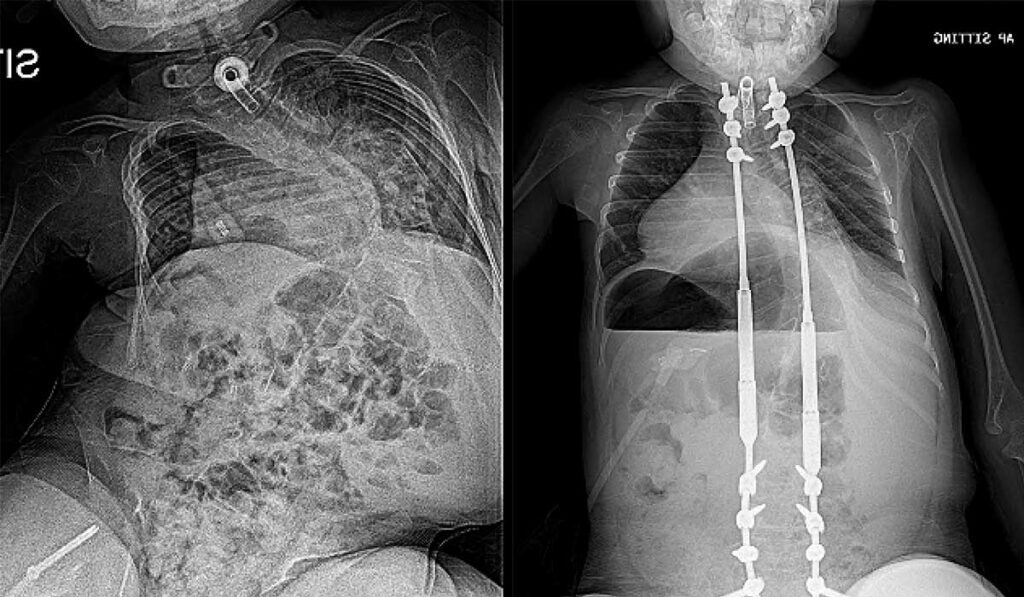
When curves exceed 90 degrees or are excessively stiff, children may be candidates for halo-gravity traction (HGT), as a precursor to definitive treatment like spinal fusion or growing rods.
HGT involves embedding pins in the skull and using a weighted pulley system to pull up on the spine to incrementally reduce curvature. “It looks barbaric,” Louer said. “But patients actually love it – they will eat more and have improved lung function.”
“We need to treat progressive curves of around 30 degrees as soon as we recognize them as being problematic – as early as one year of age.”
Studies demonstrate that preoperative HGT corrects initial Cobb angles by 24.1 and 19.3 percent in the coronal and sagittal planes respectively, with some studies reporting an average deformity correction of 35 percent. HGT also leads to safer spinal surgeries, fewer three-column osteotomies and less blood loss.
Toward Successful Treatment Decisions
Rib humps are usually the first clinical indication of spinal rotation in a young patient. “Standard screening techniques with an Adam’s forward bend test remain the mainstay of early detection in patients who are old enough to comply with instructions,” Louer said. “Clinicians should refer patients with curves of 20 degrees or more on X-ray for scoliosis evaluation.”
A successful treatment plan, Louer says, hinges on factors that include curve severity, age and maturity, nutritional status, presence of restrictive lung disease as well as social support. He stresses a treatment plan should include close collaboration with pulmonary and neuromuscular physicians to ensure all medical needs are being addressed.
Louer and colleagues in the Pediatric Spine Study Group (PSSG) are working to shape best practices by enrolling patients in PSSG’s patient registry and collaborating on research. “Because of its rarity, the most impactful research in early onset scoliosis comes from multicenter efforts. This collaboration also allows for easy transfer of ideas and drives innovation in this field,” Louer said.