Researchers in the U.S. have issued the country’s first evidenced-based screening guidelines for gastric precancer. The number of people at risk for gastric cancer is increasing as the U.S. population becomes more diverse.
“Stomach cancer really has been overlooked in the U.S.,” said Shailja Shah, M.D., an assistant professor of medicine at Vanderbilt University Medical Center. “It is a cancer that is screened for in some high-incidence countries like Japan and South Korea, with impressive declines in related mortality. The mortality reduction is the direct result of cancer detection at an early, asymptomatic stage.”
Shah was one of the lead members of the American Gastroenterology Association’s Technical Review team on gastric intestinal metaplasia surveillance for early gastric cancer detection. The team’s work formed the foundation for the new guidelines.
“Considering that more than 45 million foreign-born individuals live in the U.S., with over one million arriving annually and from areas of high gastric cancer incidence, it is pretty clear that we need to do better,” Shah said.
Precancerous Mucosal Changes
Gastric cancer is endemic in many regions worldwide, including Asian-Pacific and Latin American countries. The majority of people in these countries have been infected early in life with the bacterium Helicobacter pylori, which is generally accepted to be the primary trigger for the process that leads to the most common type of gastric cancer.
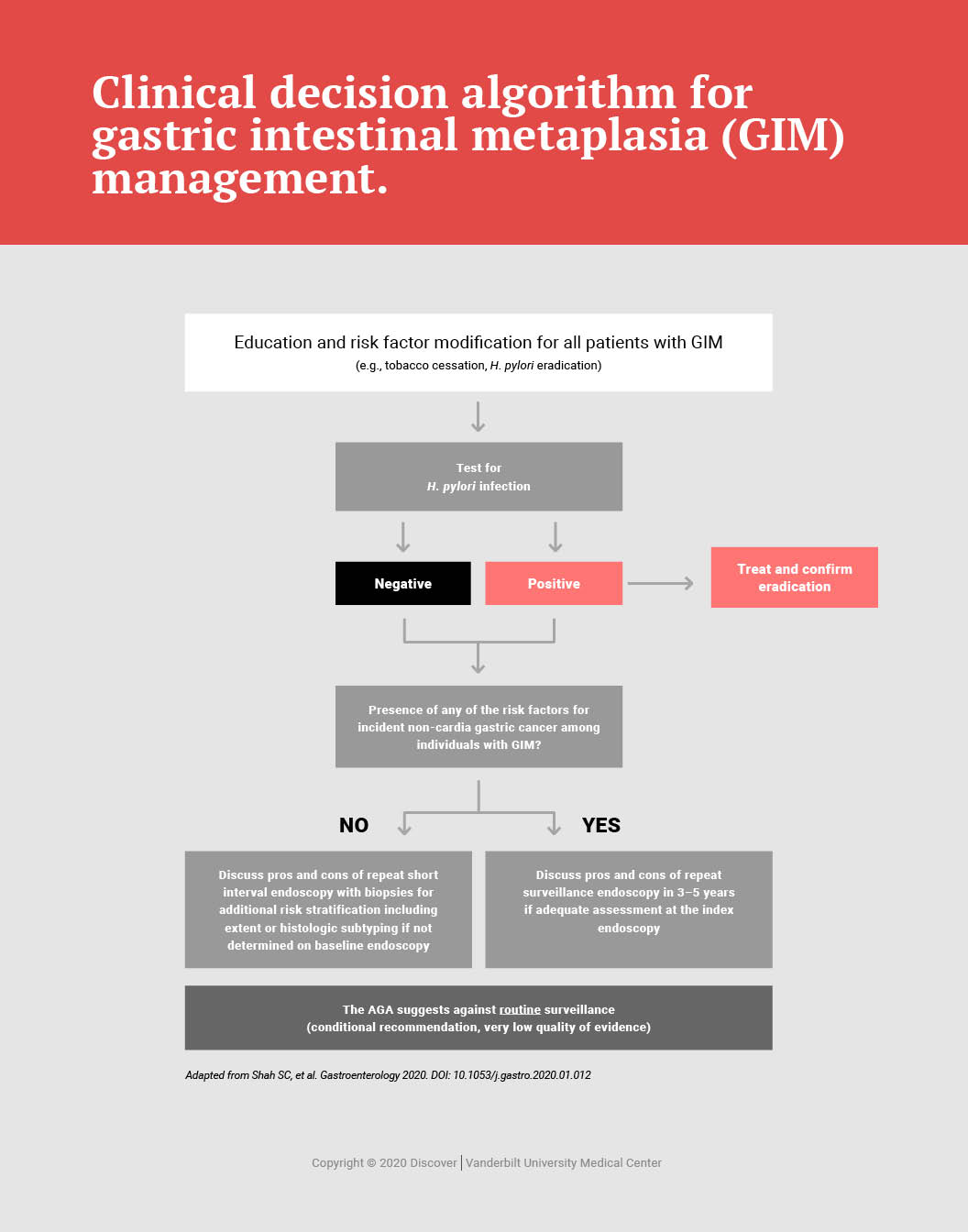
Precancerous mucosal changes, such as gastric intestinal metaplasia, might occur as a result of chronic H. pylori infection, and these mucosal changes identify someone as at a significantly higher risk for gastric cancer.
“The fact that there are precancerous mucosal changes easily diagnosed on routine histopathology is one key reason why endoscopic screening and surveillance works,” Shah said. “In a very small portion of people, these precancerous changes progress to cancer slowly over time, and this affords us the opportunity to diagnose cancers much earlier in these high-risk individuals.”
“The fact that there are precancerous mucosal changes easily diagnosed on routine histopathology is one key reason why endoscopic screening and surveillance works.”
Cost-effectiveness of Screening
In a seminal analysis published in Gastroenterology, Shah and colleagues demonstrated that performing upper endoscopy for gastric cancer at age 50, bundled with colonoscopy for average-risk colorectal cancer screening, is cost-effective for non-white races/ethnicities — specifically, Hispanics, non-Hispanic blacks and Asian Americans.
Shah and colleagues designed their model with the U.S. health care reimbursement structure in mind, given that anesthesia, facility fees and procedural time add substantial additional costs.
“The major cost-benefit of the model resulted from the detection of early-stage gastric neoplasia, which is most often asymptomatic, would therefore not prompt an upper endoscopy, [and] is typically curative,” Shah said.
This is in contrast to when a person starts having symptoms, such as gastrointestinal bleeding, that prompt endoscopic evaluation. “Once symptoms present, gastric cancer is typically at a more advanced stage, where therapeutic options are limited at best,” Shah said. “This is the more common scenario in the U.S. since we don’t screen.”
Serving High-risk Populations
Worldwide, gastric cancer is the fifth most common cancer and a major cause of cancer-related death. In the U.S., gastric cancer ranks fifteenth among cancers. Shah notes the prevalence of H. pylori infection is much lower in the U.S. than it was decades ago because of factors including improved sanitation and effective therapies for H. pylori eradication.
“It is still the most common chronic bacterial infection worldwide,” Shah said. “While the U.S. is generally considered a low prevalence country, there are clear differences based on the population.” Factors other than chronic H. pylori infection that can put people at increased risk include diet, smoking and family history, Shah said.
Shah is collaborating with a team of investigators nationally to compile evidence to lobby for formalized national gastric cancer screening guidelines for high-risk populations, including racial/ethnic minorities and immigrants from countries where gastric cancer is endemic. The effort may help standardize selection criteria, Shah said, and secure insurance coverage for upper endoscopy as part of routine cancer prevention and healthcare maintenance.